1. Introduction
Modern medical science has dramatically expanded the ability to sustain human life through advanced technologies such as mechanical ventilation, artificial nutrition, and intensive care monitoring. Patients who once would have died within hours or days can now survive for months or even decades with artificial medical support. While these developments represent remarkable achievements in medicine, they have also created profound ethical and legal dilemmas. One of the most difficult questions concerns situations where a patient remains biologically alive but has permanently lost consciousness or meaningful cognitive function.
Medical conditions such as persistent vegetative state (PVS), irreversible coma, and severe neurological damage have become central to contemporary debates on euthanasia and end-of-life care. In such cases, patients are unable to communicate their wishes, leaving families, doctors, and courts to decide whether life-sustaining treatment should continue indefinitely. These decisions raise complex issues concerning human dignity, patient autonomy, medical ethics, and the limits of life-prolonging technologies.
In India, the legal dimension of these debates became prominent through landmark judicial decisions such as Aruna Ramachandra Shanbaug v. Union of India (2011) and Common Cause v. Union of India (2018). Through these judgments, the Supreme Court of India gradually recognised the concept of passive euthanasia and affirmed that the right to life under Article 21 includes the right to die with dignity in specific medical circumstances.
However, legal discussions often occur without a clear understanding of the medical realities involved. To meaningfully evaluate end-of-life decisions, it is essential to understand the medical conditions underlying such cases, the ethical principles guiding doctors, and the role of living wills and advance directives. This article explores these medical and ethical dimensions in order to clarify when life-sustaining treatment may become medically futile.
2. Disorders of Consciousness
End-of-life debates frequently involve patients suffering from severe neurological conditions known as disorders of consciousness. These conditions affect the brain’s ability to maintain awareness, cognition, and voluntary interaction with the environment.
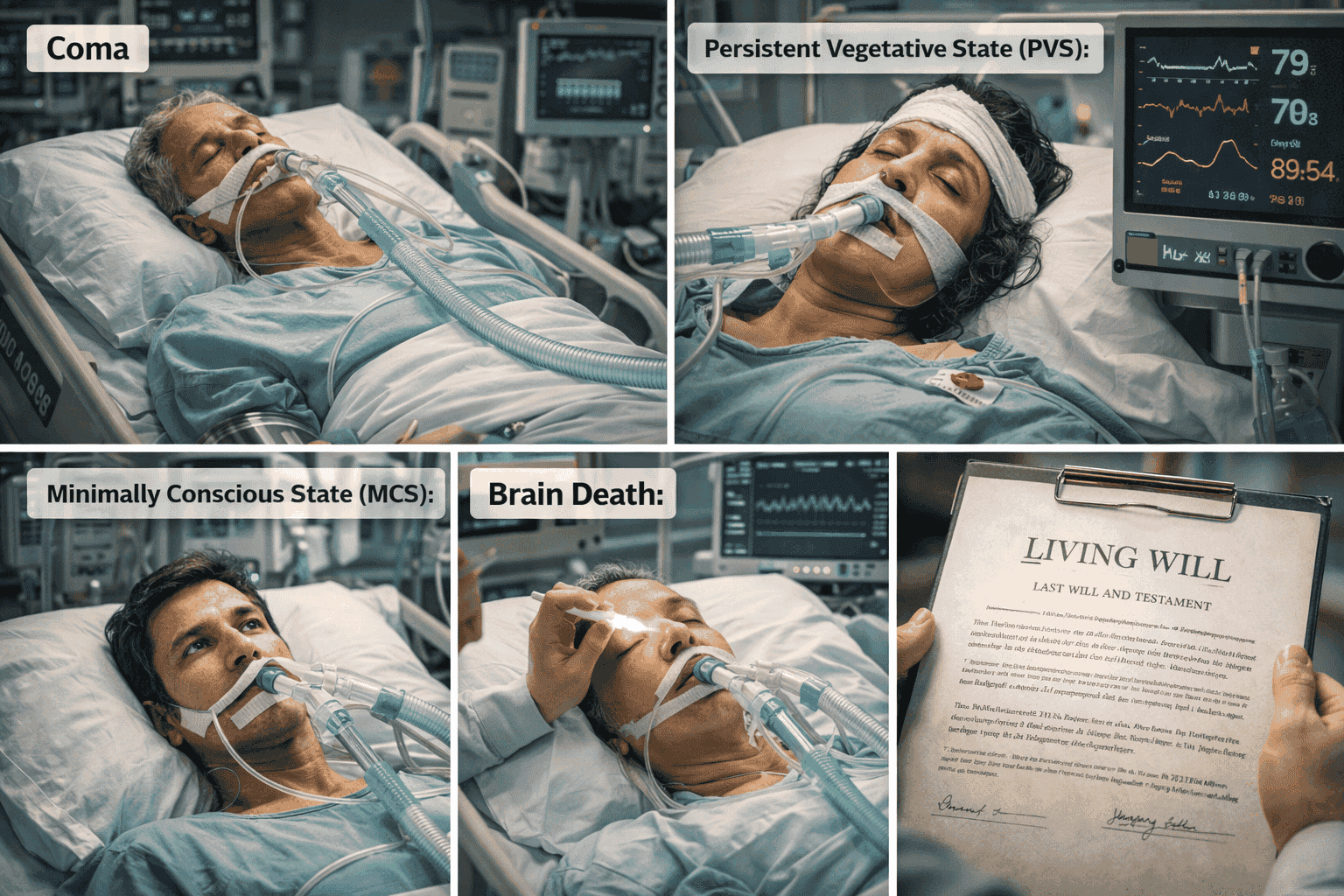
Four medical states commonly arise in legal cases involving end-of-life decisions: coma, persistent vegetative state, minimally conscious state, and brain death. Although these conditions are sometimes confused in public discussions, they differ significantly in medical characteristics and prognosis.
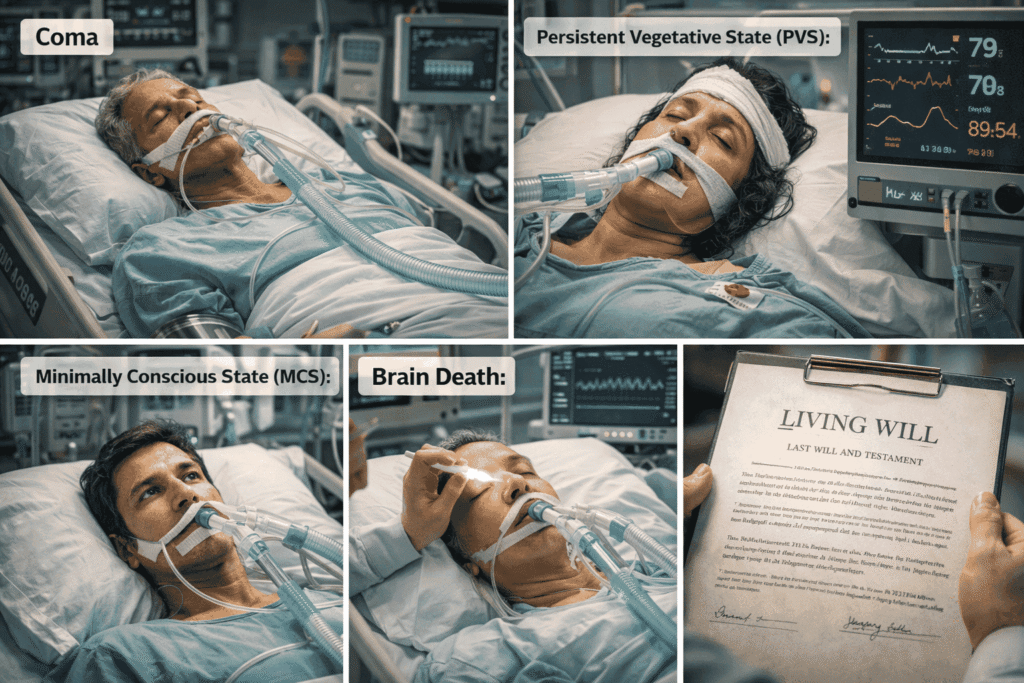
a) Coma:
Coma is a state of deep unconsciousness in which the patient shows no signs of wakefulness or awareness. Individuals in coma cannot respond to external stimuli, speak, or perform voluntary actions. Coma is usually temporary and may last days or weeks. Some patients recover consciousness, while others may transition into other neurological states.
b) Persistent Vegetative State (PVS):
It occurs when a patient regains basic wake-sleep cycles but remains entirely unaware of their surroundings. Patients may open their eyes, breathe independently, and display reflexive movements, but they show no meaningful cognitive response or conscious awareness.
c) Minimally Conscious State (MCS):
It represents a condition where patients demonstrate limited but detectable signs of awareness. They may respond inconsistently to commands, exhibit emotional reactions, or track objects with their eyes.
d) Brain Death
Brain Death in contrast, refers to the irreversible cessation of all brain activity, including brain-stem functions responsible for breathing and consciousness. Brain death is legally recognised as death in many jurisdictions, including India.
Misunderstanding these medical distinctions often leads to confusion in legal debates about euthanasia and life-support withdrawal. While brain death constitutes legal death, patients in vegetative states remain biologically alive, creating complex ethical and legal dilemmas.
3. Persistent Vegetative State (PVS)
A persistent vegetative state is one of the most challenging medical conditions involved in euthanasia debates. In PVS, the cerebral cortex, the part of the brain responsible for awareness, cognition, and personality, suffers severe and irreversible damage. However, the brain stem may continue to function, allowing basic biological processes such as breathing and sleep cycles to continue.
Patients in a vegetative state may appear awake because their eyes open and close. They may also exhibit reflexive behaviours such as limb movements or facial expressions. However, these actions occur without conscious awareness or intentional control.
Medical research indicates that the probability of recovery decreases dramatically as the duration of the vegetative state increases. After several months, particularly when caused by oxygen deprivation or severe brain injury, the chances of regaining meaningful consciousness become extremely low.
The case of Aruna Shanbaug illustrates this medical reality. Following a violent assault in 1973, she remained in a vegetative state for more than four decades before her death in 2015. During this period, she showed no signs of cognitive awareness despite receiving continuous medical care.
Cases involving PVS raise deeply troubling ethical questions. If a patient permanently lacks consciousness and the ability to experience the world, should medical treatment continue indefinitely? Does sustaining biological life without awareness truly serve the patient’s interests? These questions lie at the centre of debates over passive euthanasia.
4. Brain Death vs Coma: Why the Distinction Matters
Understanding the difference between brain death, coma, and vegetative states is essential for both medical ethics and legal policy.
Brain death occurs when the brain, including the brain stem, irreversibly ceases to function. Because the brain stem controls breathing and vital reflexes, a brain-dead patient cannot breathe independently and requires mechanical ventilation. Once brain death is medically confirmed, the person is legally considered dead.
In India, brain death is recognised under the Transplantation of Human Organs and Tissues Act, 1994 (THOTA). This recognition allows organs to be retrieved for transplantation after brain death, provided consent requirements are satisfied.
In contrast, patients in coma or vegetative states retain some brain function and therefore are not legally dead. They may continue breathing and maintaining basic bodily functions with medical assistance.
This distinction has major legal consequences. Brain-dead patients can become organ donors because death has already occurred. Patients in vegetative states, however, remain legally alive, making decisions about life-support withdrawal far more complex.
Public misunderstanding of these medical categories often complicates euthanasia debates. Some individuals incorrectly assume that vegetative state patients are already “brain dead,” which is medically inaccurate.
5. Life-Sustaining Medical Technology
Modern medicine possesses extraordinary capacity to prolong biological life through advanced technologies.
Key forms of life-sustaining treatment include:
- Mechanical ventilation, which assists or replaces breathing
- Artificial nutrition and hydration, delivered through feeding tubes
- Dialysis, which replaces kidney function
- Intensive care monitoring and medication
These technologies have saved countless lives. However, they also create ethical dilemmas when patients suffer irreversible conditions with no realistic prospect of recovery.
In such circumstances, doctors may confront the concept of medical futility. Medical futility refers to situations where continued treatment fails to achieve meaningful health improvement or recovery. In other words, treatment sustains biological processes but does not restore consciousness, independence, or quality of life.
Determining medical futility is not always straightforward. Decisions must consider clinical evidence, prognosis, and ethical considerations.
6. Medical Ethics & End-of-Life Decisions
Medical professionals rely on several ethical principles when making treatment decisions.
1. Patient Autonomy
Autonomy refers to the patient’s right to make informed decisions about their own medical treatment. Respecting autonomy means acknowledging individuals as moral agents capable of determining their preferences regarding life-sustaining care.
2. Beneficence
Beneficence requires doctors to act in ways that promote the patient’s welfare. Treatments should aim to improve health, relieve suffering, or restore function.
3. Non-Maleficence
This principle obligates healthcare providers to avoid causing harm. Continuing invasive treatment that only prolongs suffering may violate this obligation.
4. Sanctity of Life
Many ethical and religious traditions emphasize the intrinsic value of human life and the duty to preserve it whenever possible.
In end-of-life cases, these principles may conflict. Respecting autonomy may require withdrawing treatment, while the sanctity of life principle may encourage continuing it. Medical ethics therefore involves careful balancing of these values.
7. Living Wills and Advance Medical Directives
To address situations where patients cannot express their wishes, legal systems increasingly recognise living wills or advance medical directives.
A living will allows individuals to specify in advance the types of medical treatment they would accept or refuse if they become incapable of communicating their decisions.
In Common Cause v. Union of India (2018), the Supreme Court of India formally recognised the legality of advance medical directives. The Court held that individuals have the right to refuse life-sustaining treatment if they clearly express this preference beforehand.
Living wills serve several important functions:
- They protect patient autonomy.
- They reduce uncertainty for families and doctors.
- They prevent unwanted medical intervention.
The Court introduced procedural safeguards to ensure authenticity and prevent misuse, including verification by medical boards and legal authorities.
8. The “Best Interests of the Patient” Doctrine
When patients cannot express consent and no living will exists, doctors and courts rely on the best interests of the patient doctrine.
This standard requires decision-makers to evaluate what course of action best protects the patient’s welfare. Factors considered include:
- The patient’s medical condition and prognosis
- Previously expressed wishes
- Quality of life considerations
- Family perspectives
- Professional medical judgment
The doctrine attempts to ensure that decisions reflect compassion and respect for dignity rather than convenience or external interests.
9. Why These Issues Matter in Public Debate
Public interest in euthanasia and vegetative states has grown significantly in recent years. Online searches for phrases such as “vegetative state meaning” and “passive euthanasia meaning” demonstrate widespread curiosity and concern.
However, public debate often suffers from misunderstandings about medical terminology and legal principles. Confusion between brain death and vegetative states, for example, may distort perceptions of euthanasia.
Accurate medical knowledge is therefore essential for responsible policymaking. Legal frameworks governing end-of-life care must reflect both ethical considerations and scientific realities.
10. Conclusion
Medical realities play a central role in shaping legal and ethical debates about euthanasia. Advances in life-sustaining technologies have created situations where biological life can continue long after consciousness and recovery prospects disappear.
Determining when such treatment becomes futile requires careful evaluation of medical evidence, ethical principles, and patient autonomy.
Indian constitutional law has begun addressing these dilemmas through judicial decisions recognising passive euthanasia and living wills. However, meaningful implementation requires broader public understanding of the medical conditions underlying these debates.
Ultimately, the question is not merely whether life should be prolonged, but whether continued medical intervention truly serves the dignity and interests of the patient.
The next article in this series will examine global legal models of euthanasia and physician-assisted dying, comparing how different countries regulate end-of-life decisions.
Quick Summary
- Disorders of consciousness such as coma, PVS, and brain death differ significantly in medical and legal implications.
- Persistent vegetative state involves loss of awareness despite continued biological functions.
- Modern medical technologies can prolong life but may create situations of medical futility.
- Living wills allow individuals to express their wishes about life-sustaining treatment in advance.
- Ethical end-of-life decisions must balance autonomy, dignity, medical evidence, and compassion.
Life, Law and Dignity : Understanding Euthansia Series
The next article in this series would find as below:
- What is Euthanasia? Understanding the Concept, Types, and Global Legal Debate
- The Legal Journey of Euthanasia in India: From Aruna Shanbaug to the Right to Die with Dignity, The Legal Evolution of Euthanasia in India
- Vegetative State, Living Wills, and Medical Ethics: When Does Life-Sustaining Treatment Become Futile?
- The Harish Rana Case and Passive Euthanasia in India: A New Chapter in End-of-Life Law
- The Future of End-of-Life Law in India: Should Parliament Enact a Comprehensive Euthanasia Law?
References
- Tom L. Beauchamp & James F. Childress, Principles of Biomedical Ethics (7th ed. 2013).
- Helga Kuhse & Peter Singer, Bioethics: An Anthology (2d ed. 2006).
- Margaret Pabst Battin, Ending Life: Ethics and the Way We Die (2005).
- Jonathan Herring, Medical Law and Ethics (9th ed. 2021).
- Emily Jackson, Medical Law: Text, Cases, and Materials (5th ed. 2019).
- James Rachels, Active and Passive Euthanasia, 292 New Eng. J. Med. 78 (1975).
- John Keown, Euthanasia, Ethics and Public Policy, 11 Cambridge Q. Healthcare Ethics 345 (2002).
- Margaret Pabst Battin, Physician-Assisted Suicide and Euthanasia, 7 J. Med. Ethics 79 (1981).
- World Health Organization, Ethics and Health: End-of-Life Care (World Health Org. 2017).
- Government of Canada, Medical Assistance in Dying (MAiD) Legislation, Department of Justice (2016).
- Aruna Ramachandra Shanbaug v. Union of India, (2011) 4 S.C.C. 454 (India).
- Common Cause v. Union of India, (2018) 5 S.C.C. 1 (India).
- India Const. art. 21.
- Indian Kanoon, https://indiankanoon.org.